
Thoughts
Narratives and the Stigmatization of our Mental States
by
Nia Henderson
How historical narratives shape our view on mental health
What are Narratives?
Narratives guide our understanding of humanity, aid in our collective or individual healing, and consequently reveal that objectivity is a fabricated phenomenon resulting from stories shared by a dominant narrative and culture. Narratives (which I define as verbal, written, or visual storytelling that aids in our conceptualization of society) retain the richness of our lives and illuminate the context-specific, complex experiences in a way quantitative data falls short. Personal and collective narratives situate thoughts and behaviors within our complex societies while establishing a context in which people begin to understand actions and perceptions and can foster consciousness and increase empathy.
What Makes Narratives Powerful?
The narrative paradigm1 suggests that knowledge transfer is ever-present, requires no formal education, and narrativity is acquired through socialization. The power of narratives develops as people listen, exchange, and internalize stories that build a consensus and a culture of shared understanding. Dominate narratives emerge and become a habitual pattern of perception and tempt us to believe that the way things are is inevitable or the best they can be. Historically, the legitimacy of hierarchy has provided a platform for story-makers and storytellers who possess power (political/spiritual), intelligence, or a preferred heritage2. This allows narratives to act as a tool that prohibits social mobility, playing a central role in the justification of oppressing marginalized populations.
As an interdisciplinary scholar turned mental healthcare provider, I hold a specific interest in examining the narratives that exist within the discipline of psychology. What I found in my exploration illuminates narratives of mental illness (contribute to the stigmatization and unjustified exclusion of people who present with “psychological disorders.”
Narratives of Psychological Difference through Time
Deficiency narratives of people with mental illness— dating as far back as the thirteenth century—rationalized, centrally administered, and directed social control apparatuses and justified segregating individuals from surrounding communities.
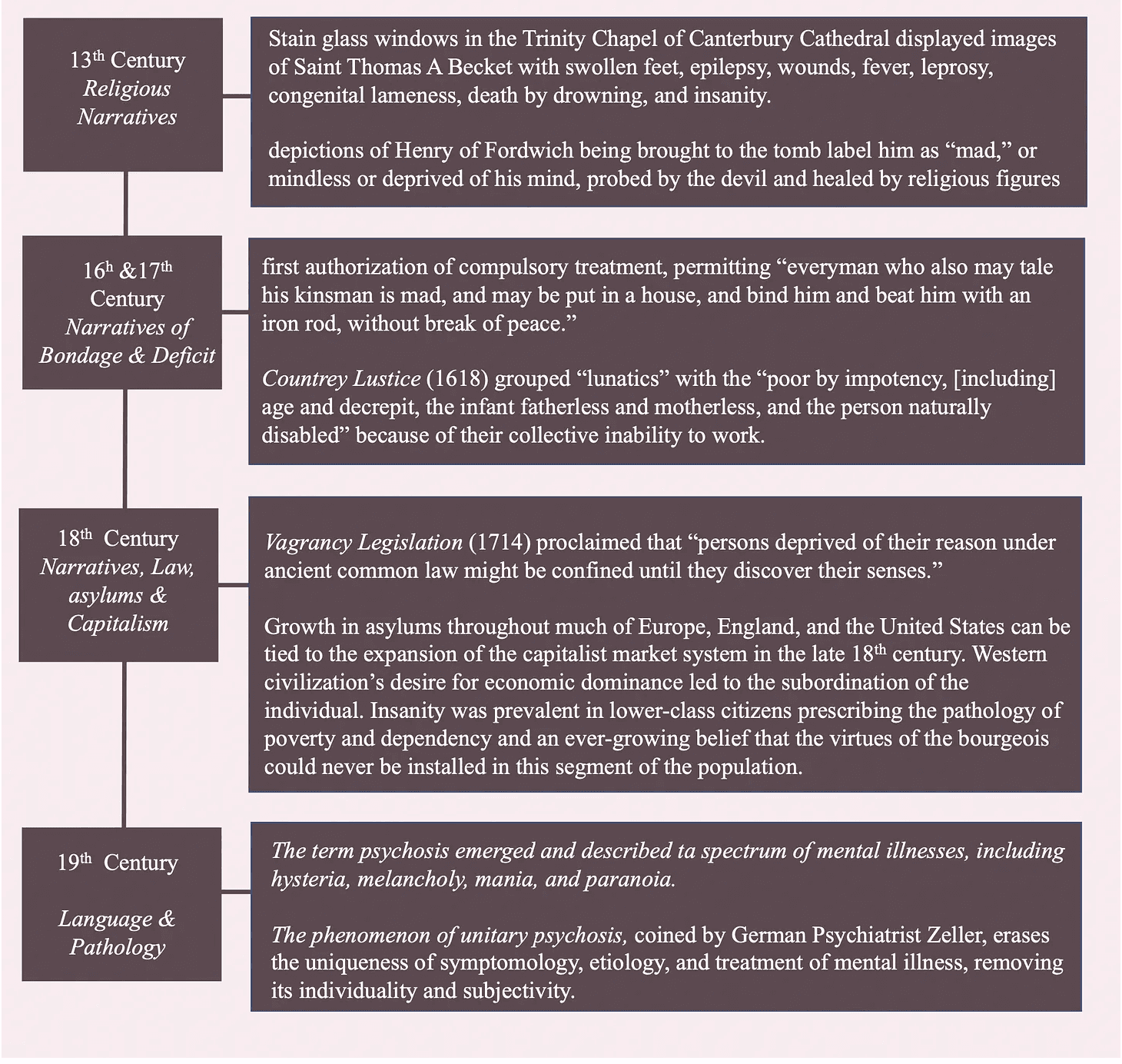
Narratives that marginalized people suffering from mental illness reach as far back as the early thirteenth century. Stain glass windows in the Trinity Chapel of Canerbery Cathedral, displayed images of Saint Thomas A Becket with swollen feet, epilepsy, wounds, fever, leprosy, congenital lameness, death by drowning, and insanity. Similarly, depictions of Henry of Fordwitch being brought to the tomb label him as “mad,” or mindless, or deprived of his mind, probed by the devil and healed by religious figures—signifying the role of religion in the formation of beliefs about the mentally ill3.
1581 marked the first authorization of compulsory treatment, permitting “everyman who also may tale his kinsman is mad, and may be put in a house, and bind him and beat him with iron rod, without break of peace.4”
Accounts of the authorization of copulatory treatment by Dalton in 1618 permitted forcible taking those that are a threat to the self and others “into a house, to bind or chain him, and to beat him with rods, and to do any other forcible act to reclaim him or to keep him so as he shall not do hurt5”
Another deficiency narrative of the “insane” is identifiable in The Countrey Lustice (1618) which grouped “lunatics” with the “poor by impotency, [including] age and decrepit, the infant fatherless and motherless, and the person naturally disabled,” because of their collective inability to work.
Later, Vagrancy Legislation (1714), proclaimed that under ancient common law, “persons deprived of their reason might be confined until they discover their senses.”
Common terms were developed to describe the “insane,” contributing to the grouping of people suffering from mental illness.
Psychosis, a term first employed by Feuchtersleben in 1845, encapsulates the changes in the entire personality and the interaction between physiological and mental processes that are a result of psychological disorder. The etiology in psychosis was due to the somatic weakness of the brain and the psychic vulnerability of the individual; and in 1892, became a term that covered the spectrum of hysteria, melancholy, mania, and paranoia6.
The phenomenon of unitary psychosis, coined by German Psychiatrist Zeller, erases the uniqueness of symptomology, etiology, and treatment of mental illness, removing its individuality and subjectivity. Most stories of the insane employ a deficiency narrative, because of the perceived inability of people with mental disorders to be productive members of society7.
This legitimized the establishment of asylums with the primary goal of socially isolating the “insane” with no intent to aid in recovery.
Asylum to The Emergence of “Helping Professions”
Growth in asylums through much of Europe, England, and the United States can be tied to the expansion of the capitalist market system in the late 18th century8. The desire for economic dominance of Euro-American civilization, lead to the subordination of the individual. “Insanity” was prevalent in lower-class citizens prescribing the pathology of poverty and dependency, and an ever-growing belief that the virtues of the bourgeois could never be installed in this segment of the population.
Andrew Scull asserts that “the careful differentiation of different sorts of deviance and the subsequent consignment of different sorts of deviance” assigned various experts; leading to “the emergence of professional and semi-professional “helping occupations.9” The assignment of experts in the early to mid 19th century led to a fundamental shift from demonological, non-human, animalistic qualities of mental disorder to a naturalistic position that perceived the “mentally insane” as lacking human mechanism, making conditions potentially remediable; granting power and influence to the psychiatric profession, and scientifically legitimizing deviance.
Why this Matters (to me)
Centuries of rhetoric that emphasized the differences and deviance of the mentally ill from people in positions of power and authority, has led to the stigmatization of psychological disorder that is identifiable today. The reduction of people to their symptomology has been central to the erasure of the personal narrative of patients in asylums. This has led to a distorted interpretation of mental illness and the subordination and marginalization of people with mental health challenges.
I believe that personal narratives of individuals with mental health challenges are necessary to subvert the constructed reality, retain the humanness of people who experience mental illness, and reduce social stigma.
1Fisher, W. R. (1984). Narration as a human communication paradigm: The case of public moral argument. Communication Monographs, 51, 1-22.
2Delgado, R. (1989). Storytelling for oppositionists and others: A plea for narrative. In R. Delgado & J. Stefancic (Eds.), Critical Race Theory (71-80).
3Allderidge, P. (1979). Hospitals, madhouses, and asylums: Cycles in the care of the insane. British Journal of Psychiatry, 134, 321-34
4 Allderidge, P. (1979). Hospitals, madhouses, and asylums: Cycles in the care of the insane. British Journal of Psychiatry, 134, 321-34
5Allderidge, P. (1979). Hospitals, madhouses, and asylums: Cycles in the care of the insane. British Journal of Psychiatry, 134, 321-34
6Bürgy, M. (2008). The concept of psychosis: Historical and phenomenological aspect. Schizophrenia Bulletin, 34(6) 1200-1210.
7Bürgy, M. (2008). The concept of psychosis: Historical and phenomenological aspect. Schizophrenia Bulletin, 34(6) 1200-1210.
8Scull, A. T. (1977) Madness and segregative control: The rise of the insane asylum. Social
Problems, 24 (3), pp.337-351.
9Scull, A. T. (1977) Madness and segregative control: The rise of the insane asylum. Social
Problems, 24 (3), pp.337-351.